Urinary Retention from Medications: How Anticholinergics Can Stop You from Peeing
 Mar, 9 2026
Mar, 9 2026
Imagine sitting on the toilet for 20 minutes, pushing hard, and nothing comes out. You feel full, maybe even painful, but your bladder just won’t empty. This isn’t just inconvenience - it’s a medical emergency called urinary retention. And for many people, especially men over 65, it’s not caused by an enlarged prostate alone. It’s caused by a common medication they’re taking for overactive bladder, anxiety, or allergies.
Anticholinergic drugs are everywhere. They’re in pills for overactive bladder like oxybutynin, tolterodine, solifenacin, and darifenacin. They’re in allergy meds like diphenhydramine (Benadryl), in antidepressants like amitriptyline, and even in some sleep aids. These drugs work by blocking acetylcholine, a chemical your body uses to tell your bladder to squeeze and empty. But when that signal gets blocked, your bladder can’t contract properly. The result? Urine builds up. And if it builds up too much, you can’t pee at all.
Why Your Bladder Needs Acetylcholine
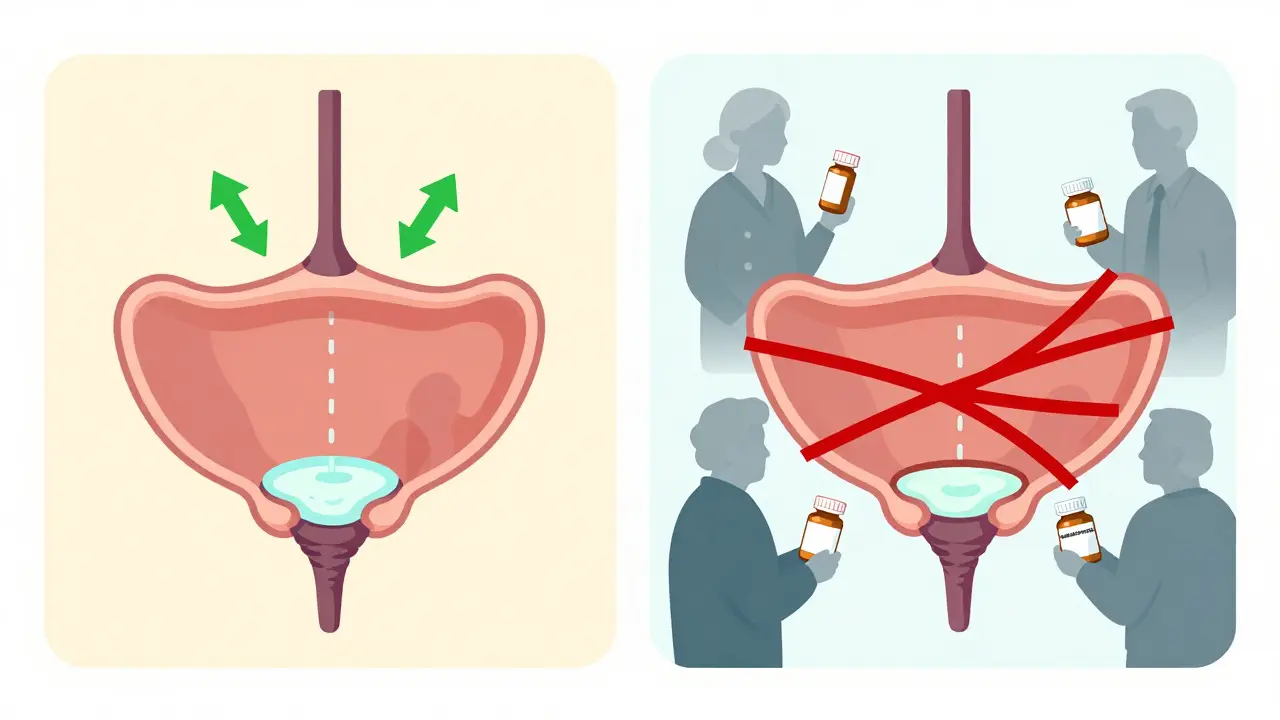
Your bladder doesn’t just fill up and wait. It’s a complex system. When it’s time to urinate, nerves send a signal using acetylcholine to the detrusor muscle - the muscle in your bladder wall. That muscle contracts, squeezing the urine out. At the same time, the sphincter muscles that hold urine in relax. This whole dance happens in less than a second in healthy people.
Anticholinergics mess with this by blocking the M3 receptors - the specific spots on the bladder muscle that respond to acetylcholine. Without that signal, the muscle doesn’t squeeze hard enough. Even if your bladder is full, it stays relaxed. That’s why you feel the urge but can’t start peeing. In severe cases, your bladder becomes overdistended, the nerves get damaged, and you lose the sensation altogether.
Who’s Most at Risk?
This isn’t something that happens to everyone. Certain people are at much higher risk:
- Men over 65 with enlarged prostates (BPH): Their bladder outlet is already narrowed. Add an anticholinergic, and the bladder can’t generate enough force to push through. Studies show this group has a 4.3% risk of acute retention - over 8 times higher than younger men without prostate issues.
- Elderly patients on multiple medications: If you’re taking 3 or more drugs with anticholinergic effects (like a sleep aid, an allergy pill, and an OAB drug), your total “anticholinergic burden” skyrockets. A 2017 study found people with a score of 3 or higher on the Anticholinergic Cognitive Burden (ACB) scale had a 68% increased risk of urinary retention.
- People with dementia or Parkinson’s: Their nervous systems are already fragile. The Beers Criteria (2019 update) lists anticholinergics as “potentially inappropriate” for older adults because they can trigger retention, confusion, and falls.
- Women with pelvic floor weakness: While less common than in men, women with prior surgeries or nerve damage can also develop retention from these drugs.
A 2022 survey of 1,234 anticholinergic users found that 8.7% had to get a catheter because they couldn’t pee. For men, that number jumped to 12.3%. For women, it was 5.1%. The difference? Prostate size. It’s not just about age - it’s about anatomy.
Which Drugs Are the Worst?
Not all anticholinergics are created equal. Some are more likely to cause retention than others.
| Drug | Primary Use | Retention Risk Level | Incidence in At-Risk Patients |
|---|---|---|---|
| Oxybutynin | Overactive bladder | High | 1.8%-2.5% |
| Tolterodine | Overactive bladder | Moderate | 1.0%-1.5% |
| Trospium chloride | Overactive bladder | Moderate-High | 1.5%-2.2% |
| Solifenacin | Overactive bladder | Moderate | 1.2%-1.8% |
| Darifenacin | Overactive bladder | Low-Moderate | 0.9%-1.4% |
| Diphenhydramine (Benadryl) | Allergy, sleep | High | Varies - up to 3x higher risk in elderly |
Why the difference? It comes down to receptor targeting. Oxybutynin blocks M1, M2, and M3 receptors - meaning it hits the bladder hard and also affects the brain and gut. That’s why it’s more likely to cause retention. Solifenacin and darifenacin are more selective - they mostly target M3, so they’re safer. But even the “safer” ones can still cause problems in vulnerable people.
The Real Cost - Emergency Rooms and Catheters
This isn’t a minor side effect. Acute urinary retention is a classic ER visit. You show up in pain, can’t pee, and they have to stick a catheter in. That’s uncomfortable. It’s expensive. And it’s preventable.
In the U.S., anticholinergic-induced retention costs the healthcare system $417 million a year in ER visits, hospital stays, and catheter supplies. The Veterans Affairs database found that 3.2% of all acute retention cases in men over 65 were caused by these drugs. When combined with opioids or other bladder-slowing meds? That number jumps to 12.7%.
One Reddit user, 71, described his ER trip after taking tolterodine: “I thought it was just constipation. Then I couldn’t pee for 18 hours. They had to catheterize me. My urologist said I got lucky - I could’ve ruptured my bladder.”
What Should You Do Instead?
If you’re on an anticholinergic and have any risk factors - especially if you’re a man with prostate issues - you have better options.
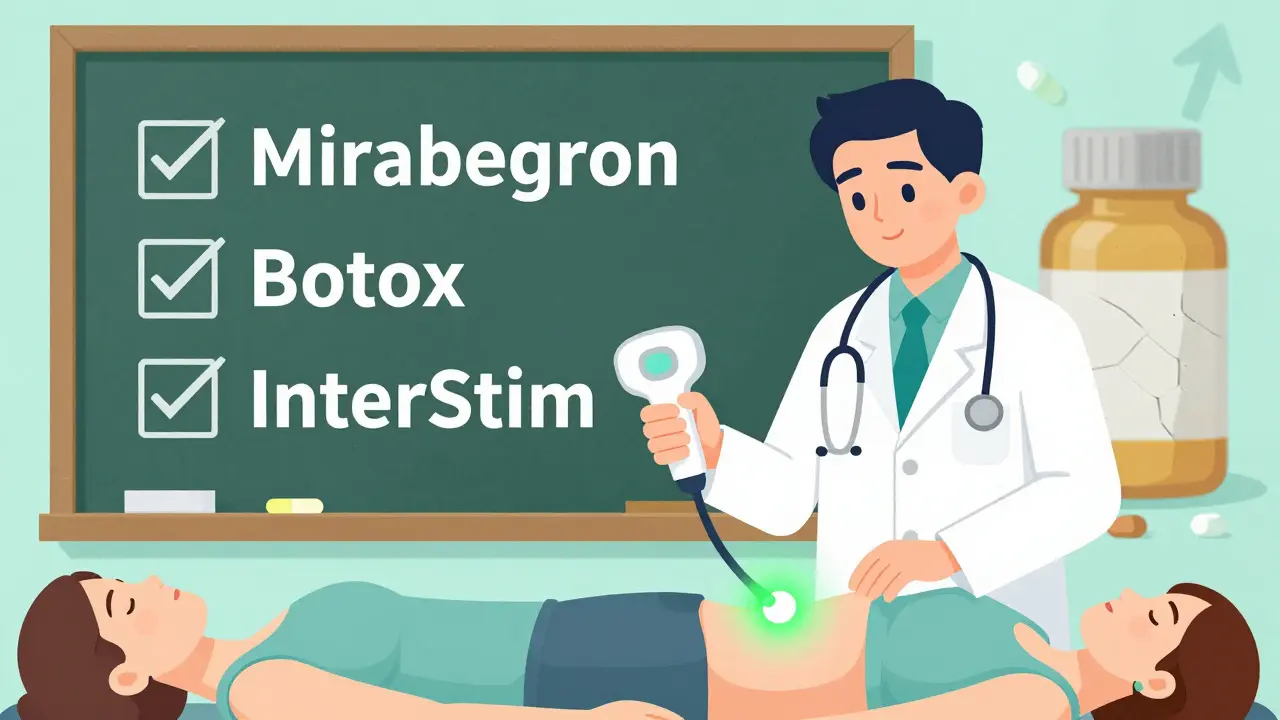
- Mirabegron (Myrbetriq): This drug doesn’t block acetylcholine. Instead, it relaxes the bladder muscle by activating beta-3 receptors. In clinical trials, it caused urinary retention in only 0.3% of users - less than a third of the anticholinergic rate.
- OnabotulinumtoxinA (Botox injections): Injected directly into the bladder wall, it temporarily paralyzes the muscle to reduce urgency. Retention risk? Only 0.5%. It’s not first-line, but it’s much safer than anticholinergics for high-risk men.
- Neuromodulation: Devices like InterStim stimulate nerves to improve bladder control. No drugs. No retention risk.
Market data shows this shift is already happening. In 2015, 58% of overactive bladder prescriptions were anticholinergics. By 2022, that dropped to 42%. Mirabegron now holds 31% of the market. Oxybutynin? Down to 18%. Doctors are learning: if you have a prostate, there’s a better way.
How to Stay Safe If You Must Take Them
Some people still need anticholinergics - especially women without prostate issues. But even then, safety matters.
- Test your post-void residual (PVR) before starting. A simple bladder scanner measures how much urine is left after you pee. If it’s over 100 mL, don’t start the drug. If it’s over 150 mL, it’s a hard stop.
- Monitor every 4 weeks for the first 3 months. Retention often happens in the first 30 days. A 2021 study found that home bladder scanners improved adherence by 92% and cut retention episodes by 61%.
- Start low, go slow. Instead of a full 5 mg dose of solifenacin, start with 2.5 mg. Wait two weeks. Check your PVR again.
- Combine with alpha-blockers if you have BPH. Drugs like tamsulosin relax the prostate and urethra. Together with a low-dose anticholinergic, they cut retention risk by 37%.
- Use patches, not pills. The oxybutynin patch delivers less drug into your bloodstream. It lowers retention risk by 42% compared to oral forms.
One patient, CathyR, shared on HealthUnlocked: “I’ve been on solifenacin for 18 months. My urologist checks my PVR every month. When it hit 150 mL, we dropped my dose. I’ve never had a problem. It’s not about avoiding the drug - it’s about watching for warning signs.”
The Bottom Line
Anticholinergics aren’t evil. They help millions of people control urgent, frequent urination. But they’re not harmless. For men with enlarged prostates, older adults on multiple meds, or anyone with a history of bladder problems - these drugs can turn a manageable condition into a medical crisis.
The guidelines are clear: Don’t give anticholinergics to someone who already can’t empty their bladder. The American Urological Association says it bluntly: “Absolutely contraindicated.”
If you’re taking one of these drugs and you notice:
- Straining to pee
- A weak or slow stream
- Feeling like you still need to go after peeing
- Needing to go more than 8 times a day
- Not peeing for 12+ hours
- stop the drug and call your doctor. Don’t wait. Don’t hope it passes. This isn’t a side effect you can tough out. It’s a blockage that can damage your kidneys and bladder permanently.
There are safer, smarter ways to manage overactive bladder - especially if you’re a man over 65. Ask your doctor about mirabegron. Ask about bladder scans. Ask about alternatives. Your bladder will thank you.
Katy Shamitz
March 10, 2026 AT 11:54I swear, my mom took Benadryl for sleep and ended up in the ER with a catheter. She didn’t even realize it was the medicine-just thought she was ‘getting old.’ Honestly, if you’re over 60 and still popping anticholinergics like candy, you’re playing Russian roulette with your bladder.
Nicholas Gama
March 10, 2026 AT 23:44Anticholinergics are just Big Pharma’s way of selling chronic problems. They don’t cure- they mask. Then you need another drug for the side effects. It’s a wheel. And we’re all stuck on it.
Mary Beth Brook
March 11, 2026 AT 03:18ACB score >3 = clinical negligence. FDA should classify these as high-risk for geriatric populations. We’re not talking side effects-we’re talking iatrogenic urinary obstruction. It’s preventable. So why isn’t it?
Neeti Rustagi
March 12, 2026 AT 20:21It is truly unfortunate that many elderly patients are not properly counseled regarding the anticholinergic burden. In India, we see this frequently-families give over-the-counter diphenhydramine without medical advice. Education is the missing link.
Dan Mayer
March 14, 2026 AT 12:29my doc put me on oxybutynin and i didnt think twice… then one morning i couldnt pee at all. like at all. i thought i was dying. turns out my bladder was full as a water balloon. they cathed me. i cried. now i take mirabegron. life is better. also i typo a lot sry
Janelle Pearl
March 15, 2026 AT 05:17I just want to say-this post saved me. My husband, 72, was on tolterodine for months. He started straining, then stopped peeing altogether. We thought it was prostate stuff… turns out it was the med. We switched to mirabegron. He’s been fine for 11 months now. Please, if you’re reading this and have a loved one on these drugs-ask about PVR scans. It’s simple. It’s safe. It’s life-changing.
Ray Foret Jr.
March 15, 2026 AT 20:58mirabegron is a game changer honestly 😊 i used to be stuck on oxybutynin and felt like a robot with a full bladder. now i can go out without panic. also-bladder scanner at home? best $200 i ever spent. no more ER trips 😅
Samantha Fierro
March 16, 2026 AT 20:15As a urology nurse practitioner, I can confirm: anticholinergic-induced retention is underdiagnosed and catastrophically under-discussed. We need mandatory PVR screening before prescribing, especially in men over 65. This isn’t anecdotal-it’s evidence-based. The data is clear. The guidelines are clear. Why aren’t we acting?
Robert Bliss
March 17, 2026 AT 16:37i didn’t know any of this. my grandpa had to get a catheter once and i thought it was just ‘old age’. now i get it. thanks for explaining. i’m gonna tell my mom to ask her doc about mirabegron. she’s on benadryl every night…
Peter Kovac
March 18, 2026 AT 06:22The $417M annual cost is misleading. It includes avoidable hospitalizations from non-compliance, poor prescribing, and patient non-adherence to PVR monitoring. The systemic failure lies in fragmented care-not the pharmacology. Fix the system, not the drug class.
APRIL HARRINGTON
March 18, 2026 AT 08:26so i took solifenacin for 2 years and then one day i just couldnt pee and i thought i was gonna die like literally i was screaming in the bathroom and my husband called 911 and they came and stuck this huge tube in me and i was sobbing and they said if we waited another hour my bladder might have burst and i just want to say if youre on this stuff and you feel like you cant go you need to go to the ER dont wait dont be brave dont be tough its not worth it
Leon Hallal
March 19, 2026 AT 02:38I’ve been on oxybutynin for 5 years. Never had a problem. My bladder’s fine. This post is fearmongering. If you’re scared of peeing, maybe don’t drink so much water.
Judith Manzano
March 19, 2026 AT 07:37This is so important. I’ve been researching bladder health since my mom had retention. I didn’t realize how many common meds contribute. Now I check every OTC pill for anticholinergic effects. It’s changed how I manage my own health.
rafeq khlo
March 20, 2026 AT 22:10Western medicine is built on suppression not cure. Anticholinergics are a symptom bandage. The real issue is pelvic floor dysfunction, neurodegeneration, and poor hydration. You’re treating the symptom while ignoring root causes. This is why we have epidemics.
Morgan Dodgen
March 22, 2026 AT 04:46Who funds these studies? Pharma? Of course they downplay retention risk. They make billions on these drugs. The real data? Hidden. The 8.7% stat? Probably 20%. They don’t track catheterizations in outpatient settings. This is a cover-up. And you’re all being played.